drvaziri@leadingdental.com
Leesburg FL, 34788
We are located in the Shoppes of Lake Village









Office Hours
9a-5p Monday through Thursday
Treatment
Mini Implants
MINI DENTAL IMPLANTS
OUR SMALL WONDER making a BIG difference in peoples lives.
Unable to eat what you want?...Dentures shift, tilt and wander? Tired of messy denture pastes?...Trouble speaking clearly?...Have a fear of smiling?

We've got the solution!
"The MINI DENTAL IMPLANT"
Visit us in the morning and have the "Mini-Implant System" placed in less than two hours, then go out and enjoy your favorite lunch. Eat comfortably, have a pleasant conversation, laugh and talk with confidence. Your denture feels secure and is being held firmly in place. And all of this at an affordable price. Sounds to good to be true...but it is true! Call today for a free consultation and no obligation quote to see if you are a candidate for this revolutionary procedure.
What are Mini Dental Implants?

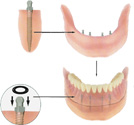
The MDI System consists of a miniature titanium implant that acts like the root of your tooth and a retaining fixture that is incorporated into the base of your denture, The head of the implant is shaped like a ball and the retaining fixture acts like a socket that contains a rubber O-ring. The O-ring snaps over the ball when the denture is seated and holds the denture at a predetermined level of force. When seated, the denture gently rests on the gum tissue. The implant fixtures allow for micro-mobility while withstanding natural lifting forces.
Who can place dental implants?
Implant placement is not yet a recognized specialty. Therefore a general dentist can perform this procedure. However this is a relatively complex procedure, and you should question the dentist’s experience.
How long does it take for the implant to heal and the false tooth placed?

Normally about 3 months. In some instances it may take 4-6 months. However a new mini implant procedure is now available that provides immediate benefits. This new mini implant procedure is minimally invasive with a short recovery time is more affordable and is being used to immediately stabilize dentures.
Is the Mini Dental Implant FDA approved?

Yes, after providing satisfactory technical and clinical evidence to that agency that the product was safe for public use and in fact had beneficial attributes, the FDA granted its formal consent to market the Mini Dental Implant device not only as a transitional or temporary dental product, but significantly, as a long-term item. (IMTEC was the first company to receive long-term approval of its Mini Dental Implants from the FDA, and for several years was the only company to have that distinction).
What is the primary and most effective use for Mini Dental Implants?

The unique design is for denture stabilization. There are approximately 50,000,000 people in the United States who are "edentulous" (literally meaning lacking teeth) who struggle daily with prosthetic devices. A majority suffer a great deal of discomfort as a result of loose or ill-fitting dentures. Many denture wearers simply withdraw from any type of social engagement as a result of being compelled to wear them. Denture patients all over the world have experienced relief from loose or ill-fitting dentures from doctors who are trained to place the MDIs. Uniquely, the MDIs can be utilized to stabilize a denture in a couple of hours by a trained doctor, with the patient leaving the office with a stabilized prosthesis.
How are the Mini Implants placed and is there major surgery involved?
No, there is no major surgery involved. The Mini Dental Implant is designed to be placed straight through the tissue into the bone. Once the implant is engaged into the bone the implant is self tapping and with special tools used to place the implants the procedure takes less than 30 minutes. Then 30 minutes later after fitting the o-ring housings into the denture, you are able to go and enjoy a light meal an hour or so after having the Mini Dental Implants placed.
TopCrowns & Bridges
Crowns are dental restorations otherwise known as "caps" which are coverings that fit over teeth. Crowns are made of natural looking porcelain and are made to improve your overall smile or to blend in with your own teeth. Sometimes an underlying metal shell is used under the porcelain if additional strength is needed.Crowns may be necessary because of broken down old fillings, fractured, chipped or sensitive teeth. Crowns are also used to improve the appearance of natural teeth that are malformed, malpositioned or discolored.
Some of the indications for a crown are:
- A previously filled tooth where there now exists more filling than tooth. The existing tooth structure becomes weakened and can no longer support the filling.
- Extensive damage by decay.
- Discolorations and compromised esthetics.
- Fractures
- Root canal - After root canal, teeth tend to become brittle and are more apt to fracture. These teeth need to be protected by a crown.
- Bridges - When missing teeth are replaced with a bridge, the adjacent teeth require crowns in order to support the replacement teeth.
Crowns strengthen and protect the remaining tooth structure and can improve the appearance of your teeth. Crowns can be made from different materials which include the full porcelain crown, the porcelain fused-to-metal crown and the all-metal crown. You and your dentist will decide which type is appropriate, depending upon the strength requirements and esthetic concerns of the tooth involved.
Fitting a crown requires at least two appointments. During your first visit, the tooth is prepared for the crown, an impression or mold is made of the tooth, and a temporary crown is placed over the prepared tooth. At the subsequent visit, the temporary crown is removed and the final crown is fitted and adjusted and cemented into place.
First Appointment
The first visit begins by giving you a local anesthetic. Depending upon the type of local anesthetic used, you can expect to be numb for one to four hours. If your anesthesia should last longer, do not be concerned. Not everyone reacts to medication in the same manner. One word of caution : While you are numb, please be careful not to bite your lip or tongue. A soft diet or no meal at all while you are numb is probably a good idea. If your child has been the patient, please watch them carefully to be sure they do not play with their tongue or lip while it is numb.
Once you are numb, your dentist will prepare your tooth in a very specific way in order to maximize the retention and esthetics of your new porcelain to metal crown. After the tooth is fully prepared, we proceed with the impression stage. We used a thin piece of retraction cord which is placed around your tooth in order to get the impression material under the gum where the crown ends. Please rest assured that this small piece of cord was removed prior to the end of today's visit.
Should you experience any discomfort you can take a mild analgesic (Tylenol™, Advil™, Anacin™, etc.) as long as there is no medical contraindication based upon your medical history. Typically, you can take anything you would normally take for a headache. If the discomfort persists, please call your dentist.
Once the impression stage is completed, your dentist or his assistant will place a temporary (transitional) crown (or bridge if multiple teeth were involved) on your tooth. These plastic (acrylic) restorations are placed on teeth to protect them and the gum tissues between dental visits. The temporary cementing medium used is designed to allow the easy removal of the temporary at your next scheduled visit.
There are a couple of additional facts you should know about regarding the care of your temporary crown:
Home care is extremely important while your temporary crown is in place. The health of your gum tissue and the success of your final treatment restoration depends upon it. PLEASE do not be afraid to clean your teeth between visits. With a minimal amount of home care, you should be able to maintain the continued health of your teeth and gum tissue during the time required to fabricate your new crown.
Sometimes, even with meticulous care, temporary crowns or bridges may become loose between visits. If this should occur, please place the temporary crown or bridge back on your tooth immediately. Putting a drop of Vaseline™ in the temporary crown or bridge will very often increase the retention and hold the temporary in place until you can schedule an appointment. Once again, REPLACING THE TEMPORARY CROWN IMMEDIATELY IS VERY IMPORTANT! It only takes a short time for teeth to move if the temporary is not put back into its proper position. This could affect the final restoration significantly and may necessitate new impressions and a great deal of time. If you can not replace the temporary crown yourself, put it in a safe place and call the office. We will be happy to recement it for you at the earliest possible moment.
Second Appointment
During the second appointment the temporary crown is removed and any temporary cement is cleaned from the prepared tooth. Your dentist will fit the final crown, check for accuracy, adjust for any bite discrepancies and evaluate the esthetics. If all of these factors are acceptable, the crown is cemented to your tooth. It is not unusual for the new crown to be mildly sensitive to cold temperatures for a few weeks. However, if the sensitivity is severe, does not subside, or if the bite feels uncomfortable, contact your dentist. Further adjustments to the crown may be necessary.
We hope that this brief instruction sheet will answer most of your questions regarding crowns. Following these simple guidelines will help provide you with the finest in dental care. If you have any questions regarding this or any other procedure, please contact your dentist.
TopCosmetic Procedures
COSMETIC BONDING
Dental bonding can improve the appearance of teeth, especially teeth that have stains which can't be removed by bleaching. During the procedure, a composite plastic resin is applied to the front surface of the teeth. Dental bonding can also be used to change the shape of teeth including adding length to short teeth.
How is the Procedure Performed?
The dentist first "roughs up" the enamel (removes the shine of the enamel) of the tooth using phosphoric acid so that the composite resin will adhere to the tooth. Then, he applies the resin to the tooth and exposes it to a high intensity light which hardens the resin and seals up the "roughed up" enamel. After bonding the resin to the tooth, the dentist polishes and contours the tooth. The procedure usually doesn't require the use of an anesthetic.
VENEERS
What are Veneers?
Veneers are ultra-thin shells of ceramic or resin material that are bonded to the fronts or backs of the teeth, much in the same way that artificial fingernails are attached to the fingers. The only requirement is that the teeth be structurally sound.
Veneers are used to correct cosmetic defects on teeth or to correct the bite (the way the teeth come together). Cosmetic imperfections that can be corrected with veneers include teeth that are slightly crooked or stained. There may be gaps or chips or the teeth may be uneven. In the past, the only way to correct these or other imperfections was to cover the tooth with a crown.
BLEACHING (teeth whitening)
How can you brighten your smile?
Your wedding is coming up and you want your smile to be its brightest. Or maybe you have an important speaking engagement. Whatever the reason, tooth bleaching isn't just for the movie stars, and it isn't just for one day. Many people have had their teeth bleached, and probably millions more are thinking about it. The desire for a brighter smile with whiter teeth is very strong, and tooth bleaching safely lightens the color of the teeth, lasting for up to five years. The most effective and safest method of tooth bleaching is dentist-supervised.
How does bleaching work?
First, the dentist will determine whether you are a candidate for tooth bleaching and what type of bleaching system would provide the best results.
If you're in a hurry for whiter teeth, you may decide to have your teeth lightened immediately. Your dentist will use an in-office bleaching system while you sit in the dental chair. However, most patients choose dentist-supervised at-home bleaching, which is more economical and provides the same results.
At the next appointment if you don't choose an in-office bleaching system the dentist or hygienist will make impressions of your teeth to fabricate a mouth-guard appliance for you. The mouth-guard is custom made for your mouth and is lightweight so that it can be worn comfortably while you are awake or sleeping. The mouth-guard is so thin that you should even be able to talk and work while wearing your mouth-guard. Along with the mouth-guard, you'll receive the bleaching materials. You'll be given instructions on how to wear the mouth-guard.
Some bleaching systems recommend bleaching your teeth from two to four hours a day. Generally this type of system requires three to six weeks to complete, and works best on patients with sensitive teeth. Other systems recommend bleaching at night while you sleep. This type of system usually requires only 10-14 days to complete.
How long does it last?
Lightness should last from one to five years, depending on your personal habits such as smoking and drinking coffee and tea. At this point you may choose to get a touch up. This procedure may not be as costly because you can probably still use the same mouth-guard. The re-treatment time also is much shorter than the original treatment time.
Is Bleaching right for me?
Generally, bleaching is successful in at least 90 percent of patients, though it may not be an option for everyone. Consider tooth bleaching if your teeth are darkened from age, coffee, tea or smoking. Teeth darkened with the color of yellow, brown or orange respond better to lightening. Other types of gray stains caused by fluorosis, smoking or tetracycline are lightened, but results are not as dramatic. If you have very sensitive teeth, periodontal disease, a lot of decay, or teeth with worn enamel, your dentist may discourage bleaching.
COMPOSITE RESINS
What is a composite resin (white filling)?
A composite resin is a tooth-colored plastic mixture filled with glass (silicon dioxide). Introduced in the 1960s, dental composites were confined to the front teeth because they were not strong enough to withstand the pressure and wear generated by the back teeth. Since then, composites have been significantly improved and can be successfully placed in the back teeth as well. Composites are not only used for restoring decay, but are also used for cosmetic improvements of the smile by changing the color of the teeth or reshaping disfigured teeth.
How is a composite placed?
Following preparation, the dentist places the composite in layers, using a light specialized to harden each layer. When the process is finished, the dentist will shape the composite to fit the tooth. The dentist then polishes the composite to prevent staining and early wear.
How long does it take to place a composite?
It takes the dentist about 10-20 minutes longer to place a composite than a silver filling. Placement time depends on the size and location of the cavity. The larger the size, the longer it will take.
What is the cost?
Prices vary, but composites average about one-and-a-half to two times the price of a silver filling. Most dental insurance plans cover the cost of the composite up to the price of a silver filling, with the patient paying the difference. As composites continue to improve, insurance companies are more likely to improve their coverage of composites.
What are the advantages of composites?
Esthetics are the main advantage, since dentists can blend shades to create a color nearly identical to that of the actual tooth. Composites bond to the tooth to support the remaining tooth structure, which helps to prevent breakage and insulate the tooth from excessive temperature changes.
What are the disadvantages?
After receiving a composite, a patient may experience post-operative sensitivity. Also, the shade of the composite can change slightly if the patient drinks tea, coffee or other staining foods. The dentist can put a clear plastic coating over the composite to prevent the color from changing if a patient is particularly concerned about tooth color. Composites tend to wear out sooner than silver fillings in larger cavities, although they hold up as well in small cavities.
How long will a composite last?
Studies have shown that composites last 7-10 years, which is comparable to silver fillings except in very large restorations, where silver fillings last longer than composites.
INLAYS & ONLAYS
What are Inlays and Onlays?
Inlays and onlays can be used in the place of a filling. Unlike soft fillings, which are molded into the shape of the mouth, inlays and onlays are made in a dental laboratory and then glued to the tooth by your dentist.
An inlay sits in a hole in the tooth and an onlay sits on the tooth. They can be made tooth-colored, gold or composite. Different materials are suitable for different parts of the mouth and parts of the teeth.
You will be given a local anesthetic to numb the area and any old fillings or damaged bits of tooth will be removed.
A mold is taken of the tooth to be repaired which will guide the dental technician who is making the inlay or onlay.
A temporary filling will protect the tooth being repaired before you return to the surgery to have the inlay or onlay glued into position. Your dentist may make minor adjustments to ensure that the tooth is comfortable to bite on.
Inlays and onlays are very strong, often lasting longer than a "traditional" filling and are useful for back teeth and large repairs for front teeth where it can be difficult to make a white filling look natural.
To ensure the inlay or onlay looks natural, your dentist will be able to match the color to that of your "natural" teeth.
Dr. Vaziri and Leading Edge Dental in Leesburg, Fl would like to discuss treatment questions you may have. Please call our office 352-365-6442
TopImplants

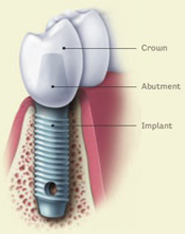
A dental implant is an artificial tooth root (Titanium) that is surgically anchored into your jaw to hold a replacement tooth or bridge in place. The benefit of using implants is that they don't rely on neighboring teeth for support, they are permanent and stable. Implants are a good solution to tooth loss because they look and feel like natural teeth. Implants now have a 95 to 99 percent success rate. They function and look just about like the real thing. This is a tremendous value to patients who don't want to have dentures.
In this diagram there is an artificial crown placed on top of the dental implant post. A dental implant goes into the jaw bone like a natural tooth root goes into the jaw bone. Look at the dental implant diagram to the right and compare the dental implant to the natural tooth root. However, the dental implant is made out of titanium metal and the natural tooth root is made out of dentin with a coating on its outside called cementum.
Who is a candidate for implants?
Virtually anyone. As long as you have sufficient jawbone in the area of the missing teeth and the bone is in good condition.

How successful are dental implants?
Many factors determine this, but if properly placed and cared for, a rate exceeding 98% can be achieved.
Who can place dental implants?
Implant placement is not recognized as a specialty so dentists, oral surgeons and periodontists all can place implants. The question is how many have they placed and how long have they been placing implants. Keep in mind when choosing a dentist oral surgeon or periodontist to place these implants not all these dentists restore the implants after having placed them. Remember the implant is just the root replacement. Dr. Vaziri and Leading Edge Dental in Leesburg, Florida has been placing and restoring dental implants over 20 years.
How long does it take to heal and restore the implant?
Normally it takes 4-6 months for conventional implants to heal then 2-4 weeks after the uncover procedure to receive the final restoration. However a new mini implant procedure is now available that provides immediate benefits. This new mini implant procedure is minimally invasive with a short recovery time is more affordable and is being used to immediately stabilize dentures and replace a single missing tooth. Call for a free consultation to see if this is for you.
TopPeriodontal Disease
HYGIENE and PERIODONTAL INFORMATION

Home care: Ideal oral hygiene can be maintained by simply brushing twice daily (am\pm) and flossing once daily, but it must be performed correctly! We recommend that a soft or ultra-soft toothbrush be used- it is our advice that you NEVER use a medium or hard toothbrush because they are too abrasive. Proper brushing is done on the inner and outer surfaces by pointing the bristles at a 45 degree angle toward the gum line and brushing in gentle circular motions. The biting surfaces are cleaned with a scrubbing motion. Proper flossing involves gently easing the floss between the teeth; then gently slipping the floss below the gum line and then easing the floss up and down (not sawing) against the teeth. Brushing and flossing are the two basics - you must do these daily.
At times the recommendation of an electric toothbrush may be a better option for optimal oral hygiene due to limited dexterity and sever gag reflexes. Plaque is the soft, bacterial bio-film which accumulates on the teeth. Once plaque remains on the teeth for a period of time it hardens into tartar or calculus. (Tartar and calculus are synonymous terms). Tartar\Calculus is hard, calcified plaque. It cannot be removed by regular home care. It can only be removed by your dentist or dental hygienist. If calculus remains untouched for a period of time you begin the process of periodontal disease.

Hygienist care: Seeing your dentist and hygienist on a regular basis is important to your overall oral health. It is recommended you see us at least two times a year for a cleaning and exam. Depending on the length of time since your last visit and the amount and location of build up you have the doctor will determine the type of cleaning you need. Stain from coffee, tea or dark staining foods and the amount of calculus build up will determine how many visits per year you will need.
X-rays are to help with the doctors diagnosis of your oral condition. The Hygienist usually takes bite-wing films once a year to maintain you oral health and monitor for decay.
Types of cleaning procedures.
Prophylaxis is a general light debris removal on the outer surface of your teeth and at the gum line. Then a polishing to smooth the surfaces of the teeth, and to remove stain and roughness.
General or Full mouth Debridement is gross removal of plaque and calculus and is performed on patients that have been more than a year without a cleaning.
Root Plane and Scaling helps eliminate the calculus build-up that cause bleeding and swelling from a gum infection. Scaling removes hard deposits (tartar) and plaque from tooth surfaces above and below the gum line. Root planing removes the hard deposits at the root surface to ensure smooth surfaces to help prevent plaque from adhering and help gum tissue re-attach and return to a healthy state. In some instances, your gum and bone tissue may not be able to return to its healthy state without the help from a periodontist due to the progression of the gum infection or periodontal disease.
There are 3 stages of periodontal disease; early, moderate and advanced.

In early periodontitis, there are pockets of 3-4 millimeters around the tooth; slight bone loss and ligament damage, and slight progression of plaque and tartar below the gum line. Gingivitis and periodontitis are inflammatory diseases of bacterial origin. Gingivitis is red, bleeding, swollen gums caused by plaque build-up on the teeth. Left untreated, gingivitis may progress to periodontitis; however, with good oral hygiene and effective plaque control, gingivitis is completely reversible. Periodontitis once known as pyorrhea, involves destruction of the gums and bone and, if left untreated, may result in tooth loss. Periodontitis, unlike gingivitis is irreversible; that is, once the damage to the gum and bone occurs, it cannot be completely undone, Fortunately, though, the disease can be arrested.


In moderate periodontitis, there are pockets of 5-6 millimeters around the tooth; up to 1\4 of the bone holding the tooth in is lost, and significant progression of plaque and tartar below the gum line.
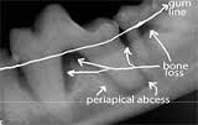
In advanced periodontitis, there are pockets of greater than 6 millimeters around the tooth; more than 1\4 of the bone holding the tooth is lost and the teeth may begin to loosen at this stage.
TopDentures & Partials
YOUR NEW DENTURE: You've just received your new dentures, and whether you're a seasoned veteran or a new denture wearer we're sure there are many questions which may need to be answered. We hope that the following information will prove to be helpful during the next few weeks of your denture adjustment period.
Learning to wear your new denture can take time! Don't become discouraged if you find some difficulty in the beginning. YOU'RE NOT ALONE! Please do not listen to friends who tell you how easy it was for them to get used to their new denture and how they can eat everything and anything. They are either bragging, have greater bone and gum support, or their memories may be poor. Your dentist will help you through any difficulties you may face or any situations that may arise during your adjustment period.
A lower denture usually takes more time to adjust to than an upper denture. The tongue may feel restricted and will tend to play, sometimes even subconsciously, with the new prosthesis. Soon your tongue will adapt to the restrictions and the new feelings that a denture presents.
Try to eat only soft foods for the first couple of days. Then, as you progress to more solid food try to eat slowly, and deliberately, attempting to place even amounts of food on both sides at the same time during the chewing cycle. By placing food on both sides of the mouth at the same time, you balance the biting forces on the new denture and will help to make it more stable. The longer you take to eat your meal, the faster you will learn to master your new prosthesis.
It is perfectly normal to experience some discomfort associated with sore spots during the adjustment period. Nature did not intend for us to wear hard plastic against soft gum tissue. It takes a while for the gum tissues to firm up and to accommodate to the hard plastic denture.
If sore spots should develop (and in some cases they do,) please continue to wear the denture and call your dentist for an adjustment appointment. This allows the dentist to see the sore area visually and make adjustments to the denture according to where the sore spots are located.
An unclean denture is neither healthy, attractive or comfortable. Clean your new denture every morning and night with either a denture toothbrush and denture toothpaste (if necessary any toothpaste can be used) or with one of the commercially available denture cleaners. Please be sure to check with your dentist to make sure that the commercial cleaner will not interfere with the denture liner you may have in your prosthesis. Permanent soft liners and temporary soft-liners react poorly to most commercial cleaners.
We prefer that you leave out one or both of your dentures at night. This allows your gum tissues to breathe and also relieves them of the constant pressure of mastication. When left out of the mouth, all dentures should be left in water to prevent the denture from warping.
Removable partial dentures
An important step in maintaining a healthy smile is to replace missing teeth. When teeth are missing, the remaining ones can change position, drifting into the surrounding spaces. Teeth that are out of position can damage tissues in the mouth and adjacent teeth. In addition, it may be difficult to clean thoroughly between crooked teeth. As a result, you run the risk of tooth decay and periodontal (gum) disease, which can lead to the loss of additional teeth.
A removable partial denture fills in the space created by missing teeth and fills out your smile. A denture helps you to properly chew food, a difficult task when you are missing teeth. In addition, a denture may improve speech and prevent a facial muscles from sagging by providing support for lips and cheeks. Partials also will help the opposing teeth from super-erupting (drifting downward). And if you are having stomach or intestinal problems, missing teeth and improper chewing my be the cause.
Removable partial dentures usually consist of replacement teeth attached to pink or gum-colored plastic bases, which are connected by metal framework. Removable partial dentures attach to your natural teeth with metal clasps or devices called precision attachments.
Precision attachments are generally more esthetic than metal clasps and they are nearly invisible. Crowns on your natural teeth may improve the fit of a removable partial denture and they are usually required with attachments. Dentures with precision attachments generally cost more than those with metal clasps. Consult with your dentist to find out which type is right for you.
How long will it take to get used to wearing a denture?
For the first few weeks, your new partial denture may feel awkward or bulky. However, with time you will eventually become more accustomed to wearing it. Inserting and removing the denture will require some practice. Follow all instructions given by your dentist. Your denture should fit into place with relative ease. Never force the partial denture into position by biting down. This could bend or break the clasps.
Relines
Gum tissues are in a constant state of change-but dentures are not! Therefore periodic relining may be necessary. If you find your denture/partial getting loose and mastication more difficult, this may be a sign that a reline may be needed. It is very important for your dentist to see you regularly to evaluate the state of your oral tissues and to determine if additional treatment is required. Dentures typically need to be relined or remade every 3-5 years. Teeth may become worn from chewing over time and a new denture or partial may be recommended. With partials, sometimes the framework still fits but the teeth are worn; therefore simply changing the teeth may be recommended. All are subject to what is the best for you and recommended by your dentist. Most lower dentures however are not the most stable to wear due to the lack of support and suction like the upper denture. If you are not happy with your lower denture see mini dental implants.
Never try to adjust your dentures yourself! Home remedies, although simple, will only lead to trouble. If any problems arise, or if you have any additional questions, your dentist is always available to help.
IMMEDIATE DENTURES
You have been advised to have an Immediate Denture, but what is it and how is it done? We hope that this information will help to explain the concepts and clear up any of the questions you might have regarding this type of prosthesis.
Let us explain what an immediate denture is by using an example: Suppose, for instance that you have eight (8) remaining upper teeth. These teeth are , unfortunately, in poor condition and cannot be utilized in any way to support a new prosthesis. If you were to have a traditional denture made, it would be necessary to have all of these teeth extracted first, the bone and gums would have to heal and then a denture could be fabricated. This process could take several weeks, if not longer, and for that time period you would have to go around without any teeth. In order to avoid this type of problem, we utilize an Immediate Denture technique. This involves taking impressions of your mouth while your teeth are still present. At the same time, when your teeth are extracted, we have a denture ready to be inserted. In this way, you never have to walk around without teeth. Immediate Dentures do present certain situations which we would like to list:
- Since we are unable to try in the denture prior to extracting your teeth, certain esthetic compromises may have to be made. This should not present any significant problem, however, and your esthetic result should be more than satisfactory.
- Since our goal is for you never to be without teeth, we will be inserting your new denture immediately after the extraction of your remaining teeth. This may seem odd, but it is perfectly normal. Typically, after the extraction of teeth, there may be some swelling. By placing your denture in immediately, this swelling can be kept to a minimum. If you did not place the denture immediately, the swelling that occurs might not allow you to wear your denture until the swelling subsided.
- It is very important that you follow the post-operative instructions of your dentist or oral surgeon very carefully. You must wear your new Immediate Denture for three (3) days, after the surgery, without removing it. This will help to control the swelling.
- Once healing has occurred, after approximately three (3) months, you will either need a reline of your existing denture, or the fabrication of an entirely new denture. If a new one has to be made, we will then he able to make any esthetic changes that you want within the limits of denture and your ridge. If a new denture is made, you will then be able to use the immediate denture as a spare (emergency) denture. This can sure come in handy if your new denture should break and need to be repaired at the laboratory.
VALPLAST and THERMOFLEX PARTIALS
A rather comfortable tooth replacement option is a flexible partial denture. These dentures are made from a composite plastic resin and can include a bio-compatible metal for superior strength in some cases. These type of partial dentures offer unique physical and esthetic properties. The Valplast partial provides lifelike esthetics, flawlessly blending with your natural tissue and surrounding dentition. The Valplast partial provides ideal adaptation to both hard and soft tissues.
Sometimes partials made need to be supported by a metal substructure so a Valplast or therma-flex type partial will be made.
Valplast® with metal rest seats has the mobility and flexibility of a non-metal thermoplastic partial with the strength of cast metal rest seats. On partial removable dentures, forces are applied to retain the denture and the supporting teeth and tissues in an aesthetic fashion. In many cases, it is proven that non-metal thermoplastics, although aesthetically pleasing, would function better if they had metal rest seats to force down pressure along the supporting teeth. The rest seats are to help support and stabilize the flexible partial. Valplast® with metal rest seats is remarkably attractive due to its natural-looking clasps and minimal metal. For patients who need a removable denture with stability and beauty.
TopWhite Fillings
Composite resins
What is a composite resin (white filling)?
A composite resin is a tooth-colored plastic mixture filled with glass (silicon dioxide). Introduced in the 1960s, dental composites were confined to the front teeth because they were not strong enough to withstand the pressure and wear generated by the back teeth. Since then, composites have been significantly improved and can be successfully placed in the back teeth as well. Composites are not only used for restoring decay, but are also used for cosmetic improvements of the smile by changing the color of the teeth or reshaping disfigured teeth.
How is a composite placed?
Following preparation, the dentist places the composite in layers, using a light specialized to harden each layer. When the process is finished, the dentist will shape the composite to fit the tooth. The dentist then polishes the composite to prevent staining and early wear.
How long does it take to place a composite?
It takes the dentist about 10-20 minutes longer to place a composite than a silver filling. Placement time depends on the size and location of the cavity. The larger the size, the longer it will take.
What is the cost?
Prices vary, but composites average about one-and-a-half to two times the price of a silver filling. Most dental insurance plans cover the cost of the composite up to the price of a silver filling, with the patient paying the difference. As composites continue to improve, insurance companies are more likely to improve their coverage of composites.
What are the advantages of composites?
Esthetics are the main advantage, since dentists can blend shades to create a color nearly identical to that of the actual tooth. Composites bond to the tooth to support the remaining tooth structure, which helps to prevent breakage and insulate the tooth from excessive temperature changes.
What are the disadvantages?
After receiving a composite, a patient may experience post-operative sensitivity. Also, the shade of the composite can change slightly if the patient drinks tea, coffee or other staining foods. The dentist can put a clear plastic coating over the composite to prevent the color from changing if a patient is particularly concerned about tooth color. Composites tend to wear out sooner than silver fillings in larger cavities, although they hold up as well in small cavities.
How long will a composite last?
Studies have shown that composites last 7-10 years, which is comparable to silver fillings except in very large restorations, where silver fillings last longer than composites.


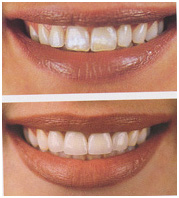
Before After
Veneers
What Is A Veneer?
Veneers are ultra-thin shells of ceramic or resin material that are bonded mainly to the front surface of the teeth, similar to the way artificial fingernails are bonded to natural finger nails. The only requirement is that the teeth be structurally sound.

Veneers are applied to correct cosmetic defects on teeth or to adjust the bite (the direction the teeth come together). Cosmetic imperfections that can be corrected with veneers include teeth that are slightly crooked or stained. There may be gaps between teeth or chipped or they may be uneven. In the past, the only way to correct these or other imperfections was to cover the tooth with a crown.
The advantage of veneers over crowns is that the teeth don't require extensive shaping prior to the procedure. Sometimes this means that little or no anesthetic is required.
Veneers made from porcelain or resin look natural. Porcelain veneers resist stains from coffee, tea or smoking better than resin veneers. On the other hand, resin veneers may be able to be made thinner and require less tooth structure to be removed before they are applied. The decision to use resin or porcelain should be made on an individual basis.
Veneers usually require three dental visits: one for a consultation and two to complete the veneers.
First:

During your first visit, your dentist will examine your teeth to make sure veneers are appropriate for you. He or she will explain what the procedure will involve and some of the limitations.
Second:
On the second visit, your dentist may need to remove up to a millimeter and a half of enamel to accommodate the thickness of the veneers. (In some cases, no enamel removal is required.) This procedure is not painful, but may be uncomfortable for some people. Your dentist will use a local anesthetic if necessary.
Third:
Next, your dentist will take a make an impression of the teeth, which will be sent to a dental laboratory. The laboratory manufactures the veneers to fit your teeth. It usually takes one or two weeks for the veneers to be made. A temporary veneer may be applied during this time.
The veneers will be applied during the third visit. Your dentist will apply them temporarily with water or glycerin first, so he or she can check the fit and color and you can see what they will look like. If the color is not quite right, the color of the veneers or the cement can be adjusted. Sometimes the veneer will need to be sent back to the laboratory to get the ideal shade.
Once you're satisfied with the veneers, your dentist will clean your teeth thoroughly and cement the veneers with bonding agents, which are hardened with a blue light.
You won't have to change the way you floss or brush. Your dentist probably will ask you to come back in a few weeks so he or she can check the veneers for any problems.
Potential problems:
If enamel is removed, your teeth can become sensitive.
The veneers may not match the color of your other teeth exactly.
Veneers may fall off. The temporary veneer is more likely to fall off because it needs to be attached in such a way that it can be easily removed.
When To Call A Professional
If your teeth seem very sensitive after having veneers put on, or if the veneers crack or fall off, contact your dentist.
TopWisdom Teeth
Wisdom teeth, or third molars, do not always erupt properly when they decide to make an appearance. It's wise to get an early opinion from your dentist on getting wisdom teeth pulled before they become impacted, causing pain, swelling, infection, cavities or gum disease.
Why don't wisdom teeth grow in right?
The shape of the modern human mouth is often too small to accommodate wisdom teeth, which make their first appearance in young adults between the ages of 15 to 25. Over the course of time, humans learned to harness fire for cooking foods and developed blade tools to better process food before consumption, they reduced the need for strong jaws to chew food.
According to studies of ancient skull specimens, over time, a full set of teeth in a smaller jaw caused crowding in permanent teeth because of lack of space.
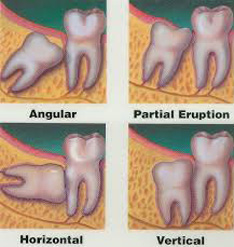
What does impacted mean?
When wisdom teeth don't have room to grow or they haven't reached their final position by age 25, they are considered impacted-no place to go and no plans to grow. Third molar impaction is the most prevalent medical developmental disorder. A full set of healthy teeth sometimes doesn't leave much room for wisdom teeth to erupt.
What kind of problems can impacted third molars cause?
Partially erupted wisdom teeth are breeding grounds for bacteria and germs that may cause infection, and cysts and tumors may grow on a trapped wisdom tooth. Jaw pain and gum disease may occur. Not all wisdom teeth cause problems, however.
Can't I just use an antibiotic?
Antibiotics only soothe infected wisdom teeth for a short time. Since people frequently use a wide variety of antibiotics, the infection may be resistant to such medication and doesn't solve the real problem: The tooth can't fit in your mouth
When is removal necessary?
It isn't wise to wait until wisdom teeth bother you. Early removal, as advised by your dentist, is generally recommended to avoid problems, such as an impacted tooth that destroys the second molar. People younger than 16 heal easier too. At an early age, people should be evaluated by their dentist who can track third molar development with the help of X-rays. Second molars should be visible to lessen the chance of damaging them during surgery. This occurs at age 11 or 12, so wisdom teeth should be removed when the decision has been made that they cannot erupt into an acceptable position.
What if I don't have any symptoms?
People with symptoms of impaction, such as pain, swelling and infection should have their wisdom teeth removed immediately. However, those with no symptoms can avoid the chance of ever suffering from the pain of impacted wisdom teeth or achieve better orthodontic treatment results by having them removed. Asymptomatic impacted wisdom teeth also should be removed to reduce the chance of unexplained pain, accommodate prosthetic appliances, or avoid cavities, periodontal disease, bone shrinkage and tumor development.
How is the tooth removed?
Surgery for impacted wisdom teeth consists of removing of the gum tissue over the tooth, gently stripping connective tissue away from the tooth and bone, removing the tooth and sewing the gum back up.
TopGum Disease
Gingivitis and periodontitis

Gingivitis and periodontitis are inflammatory diseases of bacterial origin. Gingivitis is red, bleeding, swollen gums caused by plaque build-up on the teeth. Left untreated, gingivitis may progress to periodontitis; however, with good oral hygiene and effective plaque control, gingivitis is completely reversible. Periodontitis once known as pyorrhea, involves destruction of the gums and bone and, if left untreated, may result in tooth loss. Periodontitis, unlike gingivitis is notreversible; that is, once the damage to the gum and bone occurs, it cannot be completely undone, Fortunately, though, the disease can be arrested.
There are 3 stages to periodontitis; early, moderate and advanced.
In early periodontitis, there are pockets of 3-4 millimeters around the tooth; slight bone loss and ligament damage, and slight progression of plaque and tartar below the gum line. In moderate periodontitis, there are pockets of 5-6 millimeters around the tooth; up to 1\4 of the bone holding the tooth in is lost, and significant progression of plaque and tartar below the gum line. In advanced periodontitis, there are pockets of greater than 6 millimeters around the tooth; more than 1\4 of the bone bolding the tooth in is lost and the teeth may begin to loosen at this stage.
Plaque is the soft, bacterial film which accumulates on the teeth. Once plaque remains on the teeth for a period of time it hardens into tartar or calculus. (Tartar and calculus are synonymous terms). Tartar\Calculus is hard, calcified plaque. It cannot be removed by regular home care. It can only be removed by your dentist or dental hygienist.

Home care: Ideal oral hygiene can be maintained by simply brushing twice daily (am\pm) and flossing once daily, but it must be performed correctly! We recommend that a soft or ultra-soft toothbrush be used- it is our advice that you NEVER use a medium or hard toothbrush because they are too abrasive. Proper brushing is done on the inner and outer surfaces by pointing the bristles at a 45 degree angle toward the gum line and brushing in gentle circular motions. The biting surfaces are cleaned with a scrubbing motion. Proper flossing involves gently easing the floss between the teeth; then gently slipping the floss below the gum line and then easing the floss up and down (not sawing) against the teeth. Brushing and flossing are the two basics - you must do these daily.
TopSealants
What is a sealant?
A dental sealant is a thin plastic film painted on the chewing surfaces of molars and premolars (the teeth directly in front of the molars). Sealants have been shown to be highly effective in the prevention of cavities. They were developed through dental research in the 1950s and first became available commercially in the early 1970s. The first sealant was accepted by the American Dental Association Council on Dental Therapeutics in 1972.
How effective are sealants?
Scientific studies have proven that properly applied sealants are 100 percent effective in protecting the tooth surfaces from caries. Because sealants act as a physical barrier to decay, protection is determined by the sealants' ability to adhere to the tooth. As long as the sealant remains intact, small food particles and bacteria that cause cavities cannot penetrate through or around a sealant. In fact, research has shown that sealants actually stop cavities when placed on top of a slightly decayed tooth by sealing off the supply of nutrients to the bacteria that causes a cavity.
Sealant protection is reduced or lost when part or all of the bond between the tooth and sealant is broken. However, clinical studies have shown that teeth that have lost sealants are no more susceptible to tooth decay than teeth that were never sealed.
How are sealants applied?
Sealant application involves cleaning the surface of the tooth and rinsing the surface to remove all traces of the cleaning agent. An etching solution or gel is applied to the enamel surface of the tooth, including the pits and grooves. After 15 seconds, the solution is thoroughly rinsed away with water. After the site is dried, the sealant material is applied and allowed to harden by using a special curing light. Other sealants are applied and allowed to harden much the same way nail polish is applied to fingernails.
Sealant treatment is painless and could take anywhere from five to 45 minutes to apply, depending on how many teeth need to be sealed. Sealants must be applied properly for good retention.
How long will a sealant last?
Sealants should last five years, but can last as long as 10 years. One study reported that seven years after application, an impressive 49 percent of treated teeth were still completely covered. Sealants should not be considered permanent. Regular dental check-ups are necessary to monitor the sealants' bond to the tooth.
Who should receive sealant treatment?
Children, because they have newly erupted, permanent teeth, receive the greatest benefit from sealants. The chewing surfaces of a child's teeth are most susceptible to cavities and the least benefitted by fluoride. Surveys show that approximately two-thirds of all cavities occur in the narrow pits and grooves of a child's newly erupted teeth because food particles and bacteria cannot be cleaned out.
Other patients also can benefit from sealant placement, such as those who have existing pits and grooves susceptible to decay. Research has shown that almost everybody has a 95 percent chance of eventually experiencing cavities in the pits and grooves of their teeth.
Are sealants covered by insurance?
Although insurance benefits for sealant procedures have increased considerably, coverage is still minimal. The trend is toward expanded coverage of this benefit, especially as companies start to realize that sealants are a proven preventive technique. This preventive measure can help reduce future dental expenses and protect the teeth from more aggressive forms of treatment.
TopAbscess
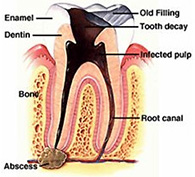
Abscess (Tooth Infection)
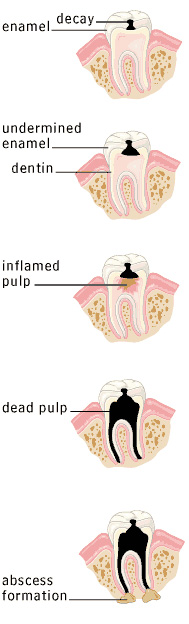
Enamel decay
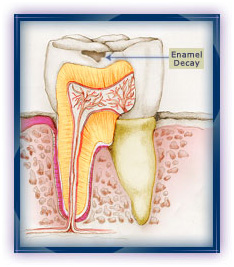
Tooth decay is a process that occurs gradually over time. It ordinarily begins at the outer layer of enamel where plaque has formed. Because enamel is almost entirely made up of minerals and has no live cells or nerves, this stage is usually painless and often goes unnoticed.
Dentin decay
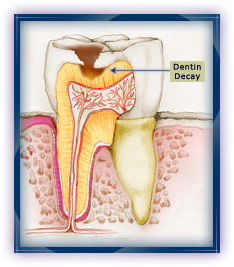
The decay then penetrates the dentin . The dentin is made up of both minerals and living cells. These cells are connected to the nerve cells in the pulp . A person may begin to notice increased sensitivity or even some pain, although this stage can also go unnoticed.
Since decay spreads faster in the dentin, the softer tissue becomes affected and cannot support the enamel. At this stage, the tooth may break and cavities can form.
Pulp decay and pulp death
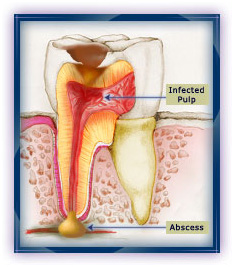
Next the pulp (the center tissue of the tooth) becomes inflamed. Left untreated, the decay will reach into the pulp, which contains pain sensitive nerve endings. The tooth will most likely ache. This requires dental assistance or the tooth may die.
Formation of an abscess
Infection causing bacteria forms an abscess, which can spread bacteria to adjoining teeth or other parts of the body. Caught early enough, the tooth can usually be saved by a root canal procedure, usually followed by a crown. If the tooth cannot be saved, it will have to be extracted.
Because the early stages of tooth decay are relatively painless and often go unnoticed, it is extremely important that you schedule an appointment with your dentist every six months for a checkup and cleaning.
TopTooth Decay
What is tooth decay, and what causes it?

Tooth decay is the disease known as caries or cavities. Unlike other diseases, however, caries is not life threatening and is highly preventable, though it affects most people to some degree during their lifetime.
Tooth decay occurs when your teeth are frequently exposed to foods containing carbohydrates (starches and sugars) like soda pop, candy, ice cream, milk, cakes, and even fruits, vegetables and juices. Natural bacteria live in your mouth and forms plaque. The plaque interacts with deposits left on your teeth from sugary and starchy foods to produce acids. These acids damage tooth enamel over time by dissolving, or demineralizing, the mineral structure of teeth, producing tooth decay and weakening the teeth.
How are cavities prevented?
The acids formed by plaque can be counteracted by simple saliva in your mouth, which acts as a buffer and remineralizing agent. Dentists often recommend chewing sugarless gum to stimulate your flow of saliva. However, though it is the body's natural defense against cavities, saliva alone is not sufficient to combat tooth decay.
The best way to prevent caries is to brush and floss regularly. To rebuild the early damage caused by plaque bacteria, we use fluoride, a natural substance which helps to remineralize the tooth structure. Fluoride is added to toothpaste to fight cavities and clean teeth. The most common source of fluoride is in the water we drink. Fluoride is added to most community water supplies and to many bottled and canned beverages.
If you are at medium to high risk for cavities, your dentist may recommend special high concentration fluoride gels, mouth rinses, or dietary fluoride supplements. Your dentist may also use professional strength anti-cavity varnish, or sealants--thin, plastic coatings that provide an extra barrier against food and debris.
Who is at risk for cavities?
Because we all carry bacteria in our mouths, everyone is at risk for cavities. Those with a diet high in carbohydrates and sugary foods and those who live in communities without fluoridated water are likely candidates for cavities. And because the area around a restored portion of a tooth is a good breeding ground for bacteria, those with a lot of fillings have a higher chance of developing tooth decay.
Children and senior citizens are the two groups at highest risk for cavities.
What can I do to help protect my teeth?
The best way to combat cavities is to follow three simple steps:
Cut down on sweets and between-meal snacks. Remember, it's these sugary and starchy treats that put your teeth at extra risk. Brush after every meal and floss daily. Cavities most often begin in hard-to-clean areas between teeth and in the fissures and pits--the edges in the tooth crown and gaps between teeth.
Proper brushing technique:
Hold the toothbrush at a 45-degree angle and brush inside, outside and between your teeth and on the top of your tongue. Be sure the bristles are firm, not bent, and replace the toothbrush after a few weeks to safeguard against reinfecting your mouth with old bacteria than can collect on the brush. Only buy toothpaste and rinses that contain fluoride (antiseptic rinses also help remove plaque) and that bear the American Dental Association seal of acceptance logo on the package. Children under six should only use a small pea-sized dab of toothpaste on the brush and should spit out as much as possible because a child's developing teeth are sensitive to higher fluoride levels. Finally, because caries is a transmittable disease, toothbrushes should never be shared, especially with your children.
See your dentist at least every six months for checkups and professional cleanings. Because caries can be difficult to detect a thorough dental examination is very important. If you get a painful toothache, if your teeth are very sensitive to hot or cold foods, or if you notice signs of decay like white spots, tooth discoloration or cavities, make an appointment right away. The longer you wait to treat infected teeth the more intensive and lengthy the treatment will be. Left neglected, caries can lead to root canal infection, permanent deterioration of decayed tooth substance and even loss of the tooth itself.
TopInlays & Onlays

Inlays and onlays can be used in the place of a filling. Unlike soft fillings, which are moulded into the shape of the mouth, inlays and onlays are made in a dental laboratory and then glued to the tooth by your dentist.
An inlay sits in a hole in the tooth and an onlay sits on the tooth. They can be made tooth-coloured, gold or composite. Different materials are suitable for different parts of the mouth and parts of the teeth.

You will be given a local anaesthetic to numb the area and any old fillings or damaged bits of tooth will be removed.
A mould will be taken of the tooth to be repaired which will guide the dental technician who is making the inlay or onlay.
A temporary filling will protect the tooth being repaired before you return to the surgery to have the inlay or onlay glued into position. Your dentist may make minor adjustments to ensure that the tooth is comfortable to bite on.
Inlays and onlays are very strong, often lasting longer than a "traditional" filling and are useful for back teeth and large repairs for front teeth where it can be difficult to make a white filling look natural.
To ensure the inlay or onlay looks natural, your dentist will be able to match the colour to that of your "natural" teeth.
TopBonding
DENTAL BONDING

Dental bonding can improve the appearance of teeth, especially teeth that have stains which can't be removed by bleaching. During the procedure, a composite plastic resin is applied to the front surface of the teeth. Dental bonding can also be used to change the shape of teeth including adding length to short teeth.
How is the Procedure Performed?
The dentist first "roughs up" the enamel (removes the shine of the enamel) of the tooth using phosphoric acid so that the composite resin will adhere to the tooth. Then, he applies the resin to the tooth and exposes it to a high intensity light which hardens the resin and seals up the "roughed up" enamel. After bonding the resin to the tooth, the dentist polishes and contours the tooth. The procedure usually doesn't require the use of an anesthetic.
How Long do the Results From Bonding Last?
Results last for 5-10 years. Bonding material does loose its shine over time, and stains and plaque easily stick to it. As the results begin to fade, bonding can be repaired or redone.
Can Dental Bonding be Removed if I am Unhappy with the Results?
Yes. However, how much the dentist "roughed up" your teeth will determine how structurally sound your teeth will be after having bonding removed.
TopSedation
Leading Edge Dental, Ali Vaziri, DMD recognizes the fact that many people have anxiety about dental visits, usually as a result of painful and lengthy procedures experienced with a previous dentist. Rather than being afraid of going to the dentist, we believe that people should be excited at the prospect of improving their appearance and health.
There are several levels of Sedation which will reduce the level of anxiety.
- Nitrous Oxide a form of conscious inhalation sedation. A very mild sense of relaxation.
- Oral Sedation a tiny pill taken orally the night prior to an appointment then 30 minutes prior to the appointment depending on the level of anxiety. Best when used for short a appointments. Once the drugs reaches it’s peak state of relaxation it begins to wear off.
- Intravenous (IV) Sedation this form of sedation is used to create a sleep like state where the patient is virtually unaware of the dentistry being performed. This technique is usually administered in the office by a specially trained and licensed dentist.
Questions about IV sedation:
Will I be completely asleep?
A lot of dental offices use terms such as "sleep dentistry" or "twilight sleep" when talking about IV sedation. This can be confusing, because it suggests that IV sedation involves being put to sleep. In reality, you remain conscious during IV sedation. You will also be able to understand and respond to requests from your dentist. However, you may not remember much about what went on because of two factors: firstly, in most people, IV sedation induces a state of deep relaxation and a feeling of not being bothered by what's going on. Secondly, the drugs used for IV sedation can produce either partial or full memory loss (amnesia) for the period of time when the drug first kicks in until it wears off. As a result, time will appear to pass very quickly and you will not recall much, or perhaps even nothing at all, of what happened. So it may, indeed, appear as if you were "asleep" during the procedure. Dr. Vaziri, Leading Edge Dental and staff will be glad to give you more information on how IV Sedation can help you with your treatment.
Is it still necessary to be numbed with local anesthetic? Will my dentist numb my gums before or after I'm sedated?
The drugs which are usually used for IV sedation are not painkillers (although some pain-killing drugs are occasionally added). While anti-anxiety drugs relax you and make you forget what happens, you will still need to be numbed.
If you have a fear of injections, you will not be numbed until the IV sedation has fully kicked in. If you have a phobia of needles, you will very probably be relaxed enough not to care by this stage. Your dentist will then wait until the local anesthetic has taken effect (i.e. until you're numb) before starting on any procedure.
What drugs are used?
Good question!! The most commonly used drugs for IV sedation are benzodiazepines. These are anti-anxiety sedative drugs the most commonly used drug for IV sedation is Midazolam (Versed). IV administered benzos have 3 main effects: they reduce anxiety/relax you, they make you sleepy, and they produce partial or total amnesia (i.e. make you forget what happened during some or, less frequently, all of the procedure.
If you have dental fears please give our office a call and we'll schedule an appointment to discuss the type of Sedation needed in your case. SEDATION "pain free dentistry while you
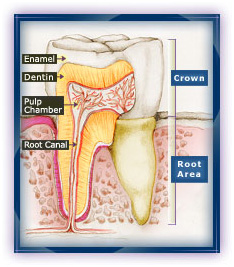
TopRoot Canals
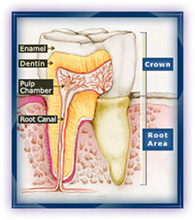
Underneath your tooth's outer enamel and within the dentin is an area of soft tissue called the pulp, which carries the tooth's nerves, veins, arteries and lymph vessels. Root canals are very small, thin divisions that branch off from the top pulp chamber down to the tip of the root. A tooth has at least one but no more than four root canals.
Why do I feel pain?
When the pulp becomes infected due to a deep cavity or fracture that allows bacteria to seep in, or injury due to trauma, it can die. Damaged or dead pulp causes increased blood flow and cellular activity, and pressure cannot be relieved from inside the tooth. Pain in the tooth is commonly felt when biting down, chewing on it and applying hot or cold foods and drinks.
Why do I need root canal therapy?
Because the tooth will not heal by itself. Without treatment, the infection will spread, bone around the tooth will begin to degenerate, and the tooth may fall_out. Pain usually worsens until one is forced to seek emergency dental attention. The only alternative is usually extraction of the tooth, which can cause surrounding teeth to shift crookedly, resulting in a bad bite. Though an extraction is cheaper, the space left behind will require an implant or a bridge, which can be more expensive than root canal therapy. If you have the choice, it's always best to keep your original teeth.
What is involved in root canal therapy?
Once your general dentist performs tests on the tooth and recommends therapy, he or she can perform the treatment or refer you to an endodontist (a pulp specialist). Treatment usually involves one to three appointments.
First, you will probably be given a local anesthetic to numb the area. Next, a gap is drilled from the crown into the pulp chamber, which, along with any infected root canal, is cleaned of all diseased pulp and reshaped. Medication may be inserted into the area to fight bacteria. Depending on the condition of the tooth, the crown may then be sealed temporarily to guard against recontamination, or the tooth may be left open to drain, or the dentist may go right ahead and fill the canals. If you're given a temporary filling, usually on the next visit it's removed and the pulp chamber and canal(s) are filled with rubberlike gutta percha or another material to prevent recontamination. If the tooth is still weak, a metal post may be inserted above the canal filling to reinforce the tooth. Once filled, the area is permanently sealed. Finally, a gold or porcelain crown is normally placed over the tooth to strengthen its structure and improve appearance.
 Top
Top